

Testicular Cancer
How is testicular cancer suspected and how is it diagnosed?
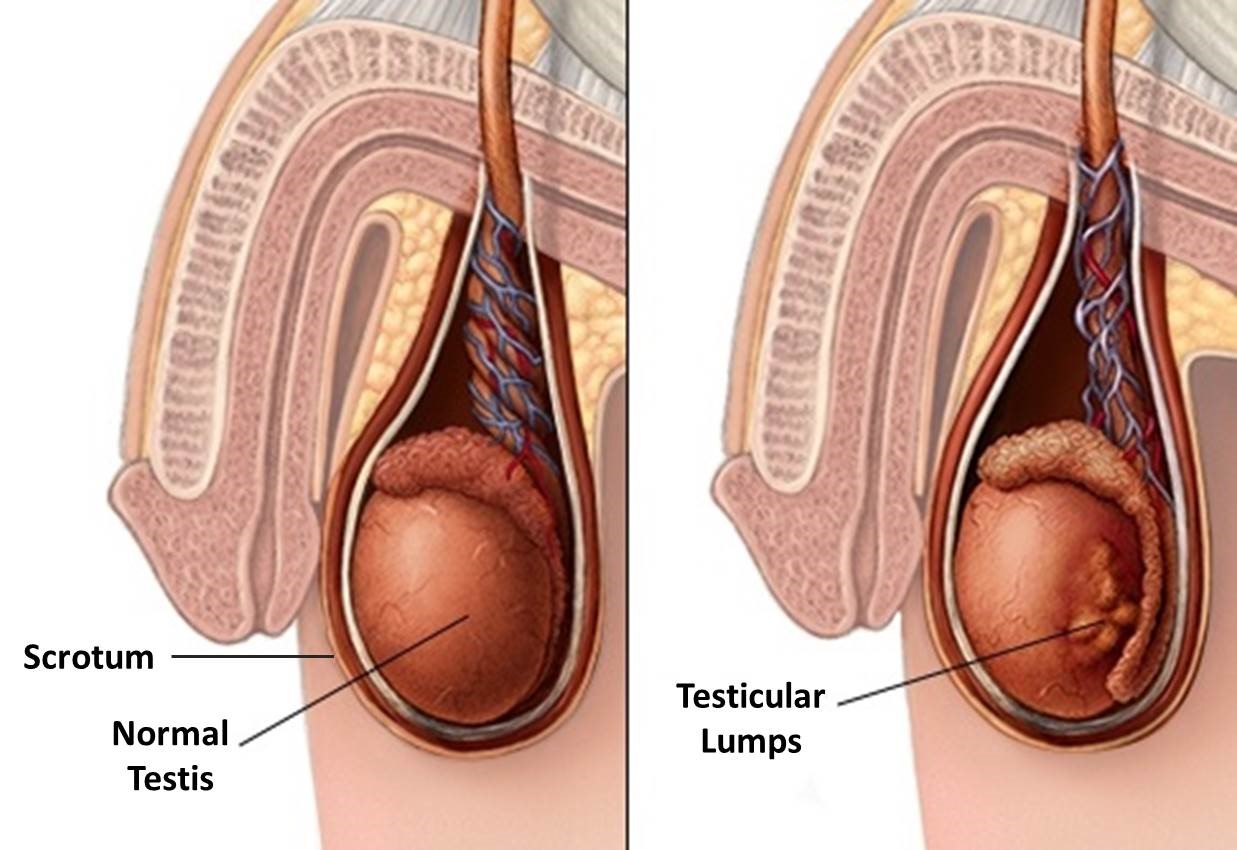
The most important and most common symptom of testicular cancer is painless swelling in the testicle. Testicle is palpable as a hard structure. Rarely, this swelling may be painful. If the tumor in the testicle causes fluid to accumulate in the scrotum suddenly, it may present as a hydrocele on examination.
In case the cancer spreads to the lymph nodes, there may be pain in the back.
Testicular cancer may also complain according to the organ it metastasizes to. For example, chest pain, shortness of breath, and cough may occur if it spreads to the lungs, which is the organ it metastasizes most often.
Scrotal doppler ultrasonography is the first imaging method to be performed in people who have testicular swelling and are thought to have testicular tumor. Ultrasonography can detect masses in the testis with high accuracy.
How is testicular cancer staged?
Clinical staging should be done before treatment and follow-up planning of testicular cancer. Thus, staging with pathology result, tumor markers (AFP, B-hCG, LDH) measured in the blood, lung films and Computed Tomography is mandatory.
Testicular cancer can occur in 3 stages:
Stage 0: Cancer cells are located only in the thin canals where sperm cells develop and are located. These cells did not spread to normal tissues. This condition, also known as “Carcinoma In Situ”, can also be named as “precancerous condition”. All tumor markers are normal.
Stage I: It is classified into 3 subgroups as Stage IA, Stage IB and Stage IS. This classification is made after the cancerous testicle is removed and examined by radical inguinal orchiectomy.
What is the Treatment for Testicular Cancer?
Treatment in testicular cancer is planned according to the stage of the disease. Surgery, chemotherapy and radiotherapy treatments can be applied. The recovery rate in testicular cancer is very high and it is pleasing.
Despite the response to the treatment applied in testicular tumors, recurrence may occur. The probability of recurrence is highest in the first 2 years. Therefore, close follow-up of the patient is very important. The risk of cancer in the other testicle of the patient is also increased. Therefore, the patient should examine his testis intermittently.
Removing the cancerous testicle does not affect the reproductive potential and sexual life of the patient. However, due to chemotherapy treatment, reproductive functions and ejaculation may be impaired.
The appearance can be improved by placing a testicular prosthesis in place of the removed testicle.
Treatment of Stage II Testicular Cancer
Treatment in stage II testicular cancer varies depending on whether the cancer is in the seminoma or non-seminoma groups.
In Seminoma, the following options are considered in treatment.
In stage 2A and 2B seminomas, after the testicle is surgically removed, radiotherapy is applied to the lymph nodes around the main vessels at the intra-abdominal level and also at the bone pelvis (hip bone) level.
In stage 2C seminomas, 3 or 4 cycles of BEP chemotherapy is given according to prognostic factors.