

BLadder Canner

What is the frequency of bladder cancer?
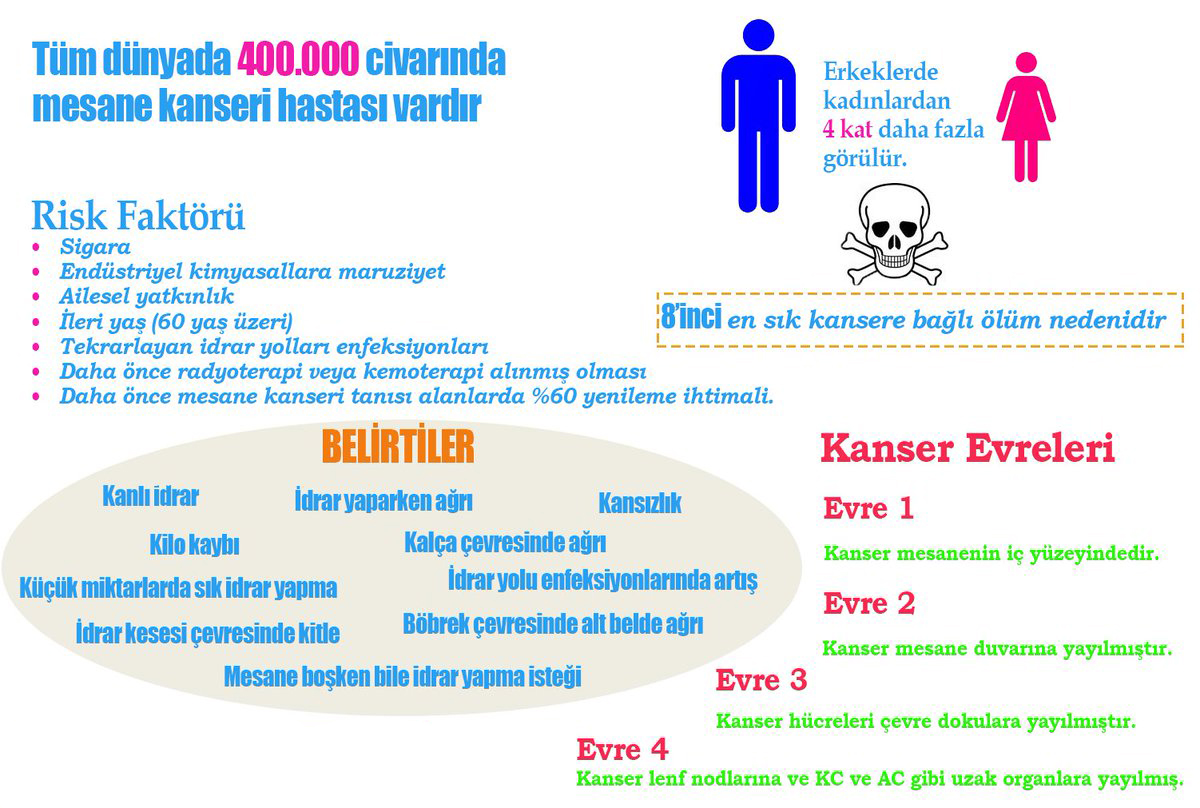
Bladder cancer is the second most common genitourinary cancer in Turkey. It is the 7th most common malignancy in men. In women, it is among the top 10 malignancies and breast cancer, which can be described as a distant relative of bladder cancer, takes the first place. According to the SEER database in the United States, the average incidence of bladder cancer is 72 years.
What are the risk factors for bladder cancer?
Due to the “aromatic amines” and “policyclic aromatic hydrocarbon” it contains, smoking is known as the strongest risk factor for bladder cancer today. Smoking is detected in half of the patients with bladder cancer.
Workers in the oil, metal, and paint industries are also at risk of developing bladder cancer due to exposure to “aromatic amines”, “policyclic aromatic hydrocarbon” and “chlorinated hydrocarbon”.
Radiation exposure increases the risk of bladder cancer. Schistosoma which is a rare bladder infection in Turkey also increases the risk of bladder cancer.
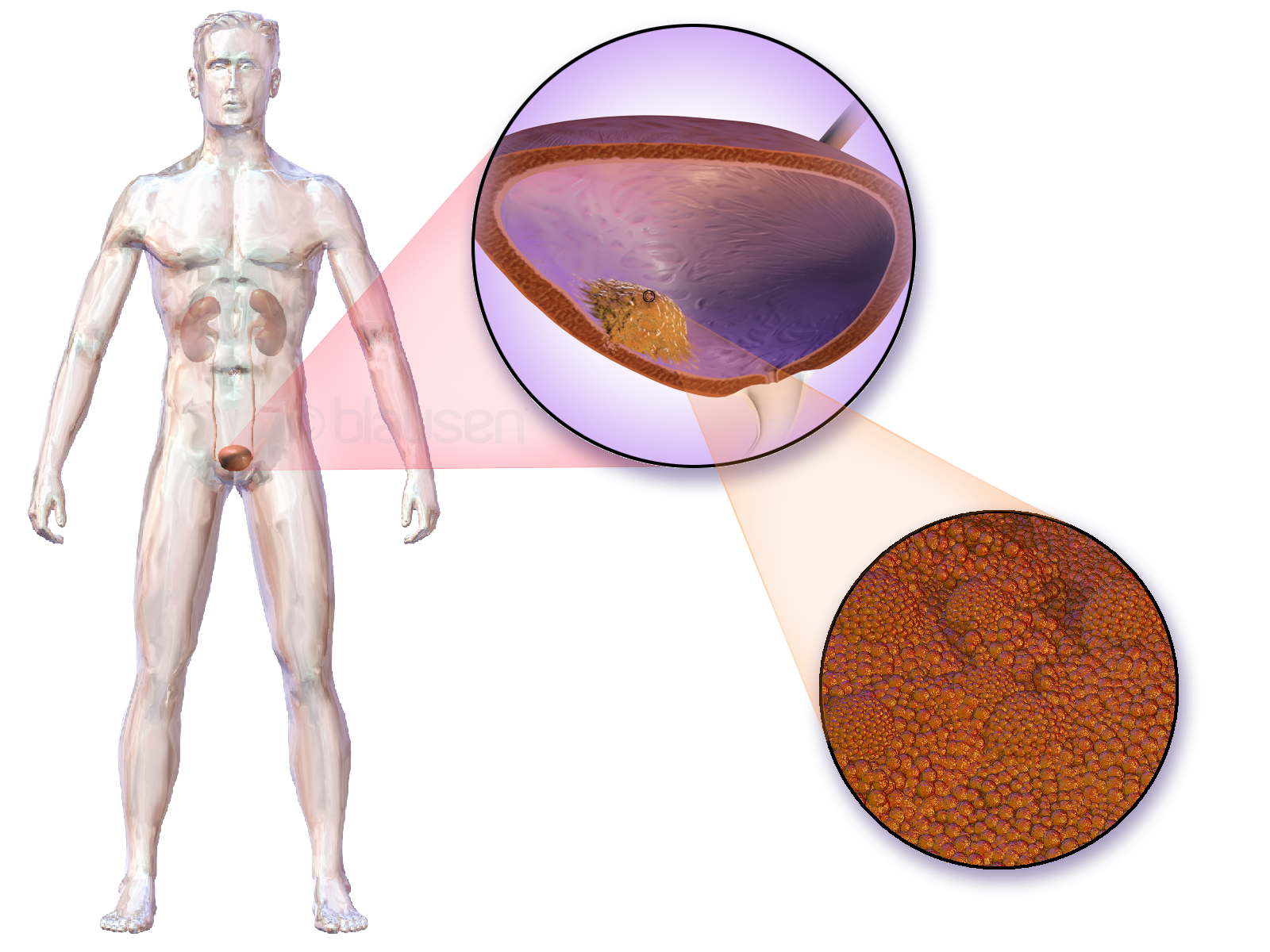
How should the approach be for a newly diagnosed bladder mass?
If a mass is detected in the bladder, the mass should be completely resected (all masses in the bladder should be scraped). Carcinoma in situ (CIS) is the pathology with the worst prognosis in non-muscle invasive bladder cancer. It has been reported that CIS is detected in the prostatic urethra in approximately 11.7% of bladder cancers, and biopsy from the prostatic urethra is recommended in risky patients. These risk factors are:
- Tumor in the bladder trigon or bladder neck
- Cases with CIS in the bladder
- Those with multiple tumors
Another important issue after TUR-B in bladder cancer is re-TUR-B, in other words, the process of scraping the tumor bed again in a second session. Studies have shown that when TUR-M was applied again to patients with pathology stage “T1”, 33-55% and 41.4% of patients with “TaG3” had residual rest tumors. That’s why TUR-B should be repeated in the following cases:
- In tumors undergoing incomplete TUR-M (which cannot be completely resected in one session due to the size of the mass)
- Tumors whose muscle tissue is not sampled in tumor examination
- In pathological stage T1 tumors
What are the risk factors for recurrence and progression in bladder cancer?
One of the most important risk factors for recurrence and progression in bladder cancer is the progression of the cancer to the detrusor muscles of the bladder. The number, size, pathological grade of the tumor such as the stage of the tumor, whether it is the first diagnosis and the accompanying CIS (carcinoma insitu) are important factors affecting recurrence and progression.
Especially CIS is very important in terms of prognosis in non-muscle invasive bladder cancers.
In muscle invasive bladder cancers, the location of the bladder at the base of the bladder, which we call the trigon, increases the likelihood of lymph node involvement and decreases survival.
Treatment in non-muscle invasive bladder cancer:
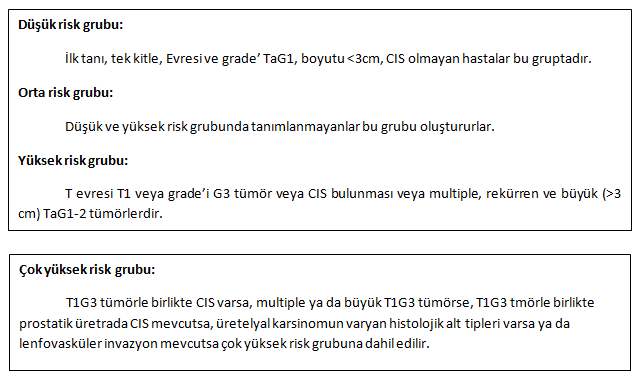
Non-muscle invasive bladder cancers are divided into low, intermediate and high risk groups and include different treatment approaches according to these risk groups.
In non-muscle invasive bladder cancers, removal of the tumor with TUR procedure can completely purify the patient from the tumor, and it often recurs or progresses in stages. Therefore, it is often necessary to add adjuvant therapy.
The possibility of recurrence and progression is low in patients in the low risk group, and intravesical chemotherapy is sufficient in the patient bed immediately after the operation. It is followed up with cystoscopy controls in the 3rd month and 1st year following the TUR surgery.
If the patients in the intermediate risk group have low expectation of recurrence (patients with an EORTC recurrence score of <5), intravesical chemotherapy (into the bladder) in the patient bed immediately after the operation is sufficient. Others are given 1 year intravesical chemotherapy or BCG. While BCG is administered weekly for 3 weeks in the 3rd, 6th and 12th months, chemotherapy still has no optimal standardization.
In patients in the high risk group, BCG application into the bladder from 1 to 3 years and cystoscopy follow-up with 6-month periods for the first 2 years and 3 months after the 5th year.
Radical cystectomy surgery should be recommended for patients in the very high risk group. In patients who are not suitable for radical cystectomy or do not accept it, 1-3 years of intravesical BCG treatment can be applied.
Radical cystectomy is the first choice treatment option in BCG-resistant bladder cancer.
Treatment in muscle invasive bladder cancer:
The most appropriate treatment option in muscle-invasive bladder cancers is complete removal of the bladder with a more radical approach. This procedure is called “Radical Cystectomy”. Urinary diversion is performed with radical cystectomy. The best alternative today for storing urine after the bladder is removed is to reconnect it to the urinary tract by making a new bladder from a part of the small intestine. This surgical procedure is called “Orthotopic Neobladder Reconstruction / Ileal Neobladder Reconstruction”.
In patients who are not suitable for neobladder or with doctor / patient preference, ileal conduit (mouthing the nascent bladder to the anterior abdominal wall) is also used in urinary diversion. Although many parts of the gastrointestinal system can be used in urinary diversion during this surgery, it is the ileum part of the small intestines (also the most preferred in our own clinic). In addition, lymph nodes up to the abdominal aorta level are routinely removed.