

Kindey Cancer
What are the prognostic factors?
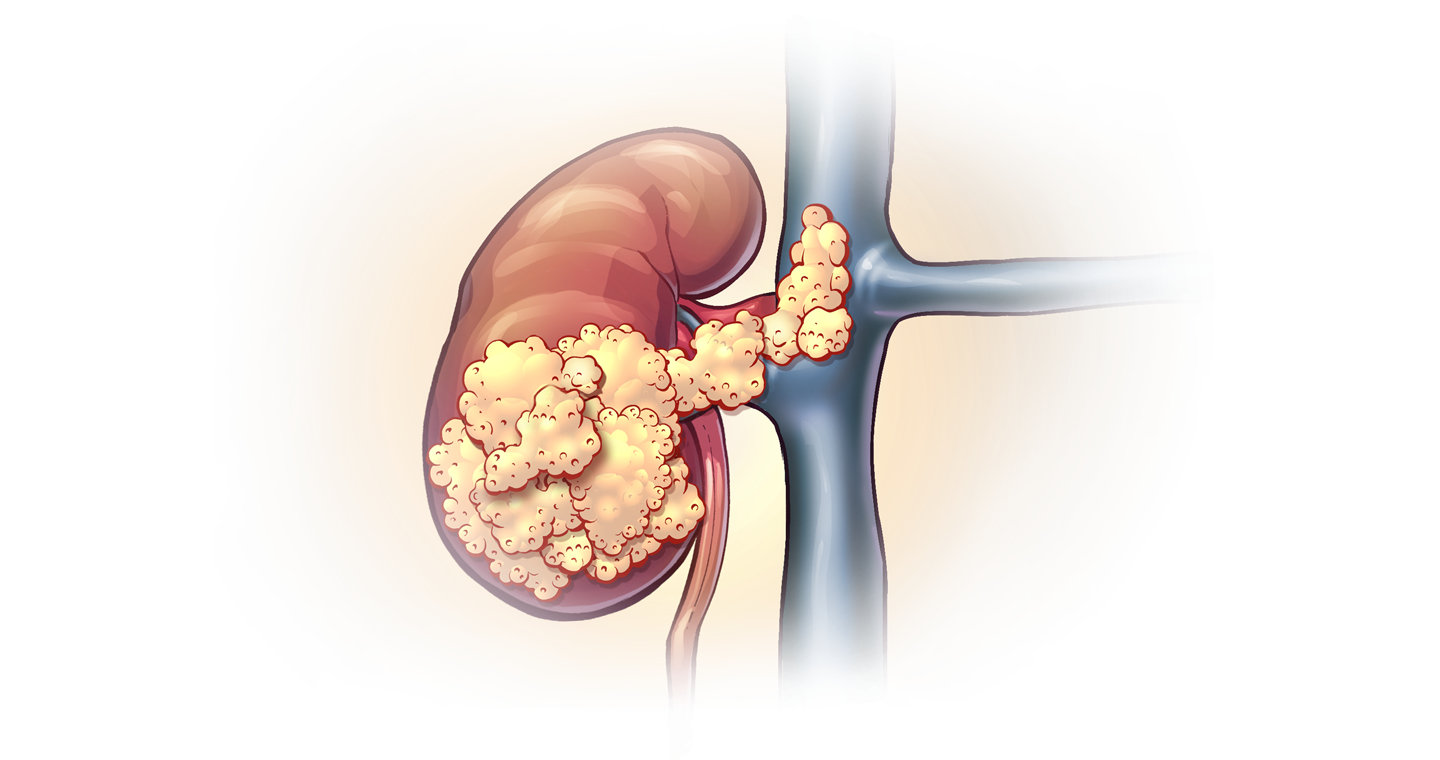
Anatomical factors: Large tumor size, venous invasion, invasion of the renal capsule, invasion of the adrenal glands, lymph nodes and spread to distant organs are poor prognostic factors.
Histological Factors: Fuhrman grade, subtype, sarcomatoid structure of the tumor, microvascular invasion, presence of necrosis in the tumor and collecting system invasion are important in prognosis.
Clinical factors: general performance of the patient, presence of local symptoms, extreme weakness, anemia, the amount of blood clot cells called platelets, the ratio of neutrophil / lymphocyte cells in the blood, C-reactive protein (CRP) and albumin levels in the blood are important indicators of prognosis.
Molecular factors: BAP1 and PBRM1 gene loss on the 3p chromosome is seen in 90% of clear cell kidney tumors with the worst prognosis and is an important risk factor for tumor recurrence. The prognosis was reported to be worse in those with specific BAP1 mutations.
T-1: Tumors <7 cm limited to the kidney
T1a: Tumor smaller than 4 cm limited in the kidney (not exceeding the kidney capsule)
T1b: Tumor limited to the kidney (not exceeding the kidney capsule) with a size of 4-7 cm
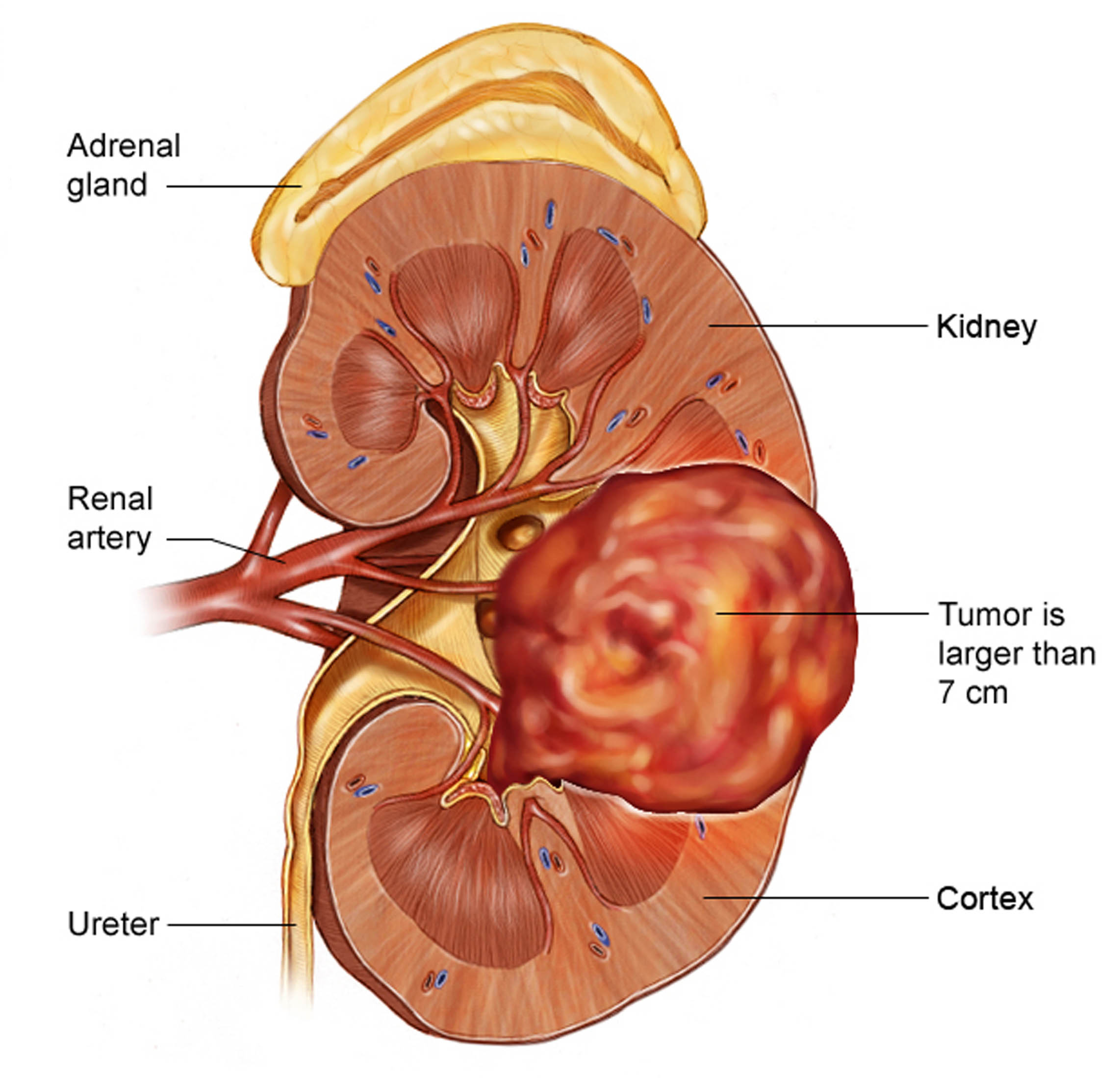
T-2: Kidney limited masses> 7 cm
T2a: Tumor limited to the kidney (not exceeding the kidney capsule), larger than 7 cm but smaller than 10 cm
T2b: Tumor diameter greater than 10 cm and not exceeding the kidney capsule
T-3: Locally advanced tumors
T3a: Tumor that has spread to the renal vein or its branches; or tumor extending into perirenal adipose tissue but not exceeding gerota
T3b: Vena cava inferior involvement below the level of the diaphragm
T3c: Vena cava inferior involvement above the level of the diaphragm, or tumor invasion of the vena cava Wall
T-4: The tumor has exceeded the membrane surrounding the adipose tissue (Gerota fascia) around the kidney.
Lymph Nodes:
Nx: Regional lymph nodes not evaluated
N0: No tumor spread in regional lymph nodes
N1: There is tumor spread in regional lymph nodes.
Distant Metastasis:
M0: Cancer does not spread to distant organs
M1: Cancer has spread to distant organs.

How is support and treatment in kidney cancer?
Surgical approach is the most appropriate to cure localized kidney cancers. Partial nephrectomy (removal of the tumor area by preserving the kidney) should be performed in tumors of suitable size and location. In T2 (> 7 cm) tumors or in patients whose localization is not suitable for partial nephrectomy, radical nephrectomy (removal of the kidney and surrounding tissues) is performed. Radical / Partial nephrectomy can be done by laparoscopic or open methods.
In locally advanced kidney cancers, it is recommended to remove the lymph nodes if lymph node involvement is detected. In vena cava thrombi, the thrombus should be removed together with the tumor kidney.
If surgery is impossible or has high risk for patient, embolization (the feeding of cancer cells is disrupted by closing the arteries leading to the tumor) may be recommended.
Active surveillance may be recommended especially in elderly patients in the presence of small kidney tumors (<4 cm). Studies have shown that when small masses are monitored, the tumor metastasizes in only 1% of patients. During the active surveillance period, the tumor is monitored with regular imaging procedures. If the tumor continues to grow, additional treatment may be required. In this case, ablation (radiofrequency- or cryo-) therapy may be a good alternative.
Ablation therapy can be performed by radiofrequency ablation (RFA) or cryotherapy. With these processes, it is aimed to kill tumor cells by heating (RFA) or freezing (cryotherapy).
Cancer diagnosis has a serious impact on the lives of patients and their relatives. It can lead to anxiety, fear and depression; It can affect your work and social life. When patients need support, they should share this with their doctor.


Treatment Options in Metastatic Kidney Cancer
If there is metastatic disease, surgical removal of the kidney (cytoreductive nephrectomy) is recommended to reduce tumor burden and alleviate symptoms. The results of the CARMENA study showed that while cytoreductive nephrectomy prolongs survival significantly in patients in the good-risk group, it does not benefit survival in patients in the moderate and poor-risk groups.
If the metastasis causes too much pain or other symptoms, additional surgery may be required to remove these metastatic tumors. Cytoreductive partial nephrectomy can be performed in patients with a single kidney or where the primary tumor is not too large and the other kidney is not working. In metastatic disease, surgery is combined with medication.
Antiangiogenic Therapy
These treatments are arranged and applied by a medical oncologist. However, treatment and follow-up with a multidisciplinary approach is very important in kidney cancers.
Antiangiogenic (tyrosine kinase inhibitors and monoclonal antibodies) drugs commonly used in kidney cancer treatment:
-Sunitinib -Pazopanib -Axitinib -Sorafenib -Tivozanib -Bevacizumab